Why accuracy is the promise—and the worry—in imaging AI
In imaging AI, “accuracy” is both the sales pitch and the clinical risk. A tool that finds more pulmonary nodules, flags intracranial hemorrhage sooner, or measures tumor change more consistently can reduce misses and speed decisions. The same tool, deployed at scale, can also create harm faster: false positives that trigger unnecessary follow-up, false negatives that delay treatment, and subtle shifts in performance across scanners, sites, and patient groups.
Part of the worry is that accuracy claims often come from controlled datasets that don’t match everyday conditions—messy histories, motion, artifacts, rare findings, and changing protocols. Even when headline metrics look strong, the real question is whether the model stays reliable in your workflow, with your prevalence, your radiologists, and a clear plan for what happens when it is wrong.
Where AI tends to help most: detection, triage, and measurement
A familiar pattern is that AI adds the most value where the task is narrow, repetitive, and time-sensitive. Detection tools can act as a second set of eyes for specific targets—lung nodules, pneumothorax, large-vessel occlusion—raising suspicion or lowering it in cases that are otherwise easy to miss at 2 a.m. Triage tools help when minutes matter: they can reorder worklists or alert teams so the most urgent studies are read first, even if the final interpretation still rests with the radiologist.
Measurement is often the most pragmatic win. Algorithms that segment organs, quantify hemorrhage volume, or track tumor size over time can reduce variability and save clicks. These gains depend on clean inputs and consistent protocols; a small change in slice thickness, contrast timing, or positioning can turn “automation” into extra review and rework.
Data quality is the ceiling: labels, modalities, and edge cases
On paper, a model’s “accuracy” looks like a property of the algorithm; in practice, it is capped by the data it was trained and tested on. Labels are the first bottleneck: if ground truth comes from a single reader, inconsistent reporting language, or short follow-up, the model learns that noise—and may look better than it is when evaluated against the same imperfect labels. Modality and protocol variety matter just as much. A tool trained mostly on one CT vendor, one reconstruction kernel, or one hospital’s contrast timing can stumble when your scanners, slice thickness, or patient positioning differs.
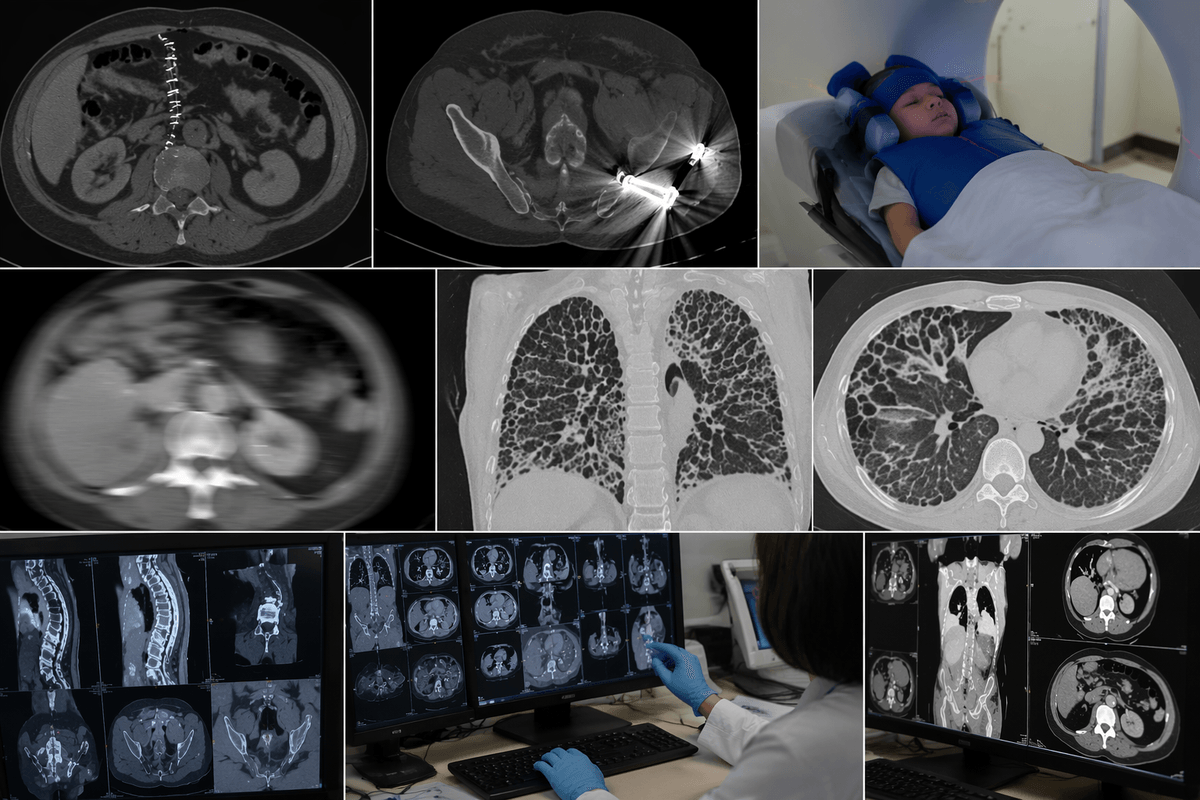
Edge cases are where the ceiling becomes visible: post-op anatomy, hardware, pediatrics, severe motion, uncommon disease, or atypical presentations. Collecting and curating enough of these examples is expensive and slow, and privacy and data-use agreements can limit how quickly a vendor can close the gap.
What’s inside the model: from classic CAD to deep learning
In day-to-day terms, imaging AI ranges from older “classic CAD” logic to modern deep learning. Classic CAD tends to rely on hand-crafted features—edges, textures, shapes—plus rules that propose candidates and then try to reject obvious false alarms. It can be easier to reason about, but it often breaks when anatomy, artifacts, or acquisition settings drift from what the rules anticipated.
Deep learning systems usually learn their own features from large image datasets, often using convolutional networks for detection and segmentation and sometimes transformers for broader context. They can be stronger across normal variation, but their failure modes can be less intuitive: a small protocol change, a different reconstruction kernel, or an unexpected implant can shift outputs in ways that are hard to predict from the UI. This is also why “explainability” often collapses to heatmaps—useful for review, but rarely a full audit trail.
How to judge “better” accuracy without fooling yourself
A common pitch is “higher AUC” or “better sensitivity,” but those numbers can hide trade-offs that matter clinically. Ask what threshold was used, whether it was fixed before looking at the test set, and what happened to specificity and positive predictive value at your expected prevalence. A model that “catches more” in a challenge dataset can still flood your service with false positives when prevalence is low, creating added follow-up, extra reads, and alert fatigue.
Study design often matters more than the headline metric. Favor external validation on sites not seen in training, with clear inclusion criteria, and with patient-level splits (not image-level) to avoid leakage across timepoints. Check whether performance is reported by scanner vendor, protocol, age, ethnicity, and whether uncertainty is shown (confidence intervals). If a tool claims it saves time, look for workflow outcomes measured prospectively; retrospective reader studies are useful, but they rarely capture integration costs, training time, and what people do when the AI is wrong.
Accuracy in real workflow: humans, UI, and failure handling
A familiar moment in deployment is when the “accurate” model still slows the reading room down. If findings appear in a separate viewer, require extra logins, or interrupt dictation, the AI’s gains get traded for clicks. Worklist triage can help, but only if it matches how your team assigns reads and handles add-ons; otherwise the “urgent” queue becomes a second inbox. Calibration matters too: a conservative threshold may miss subtle disease, while an aggressive one can create alert fatigue that trains people to ignore it.
Failure handling is where real safety shows up. Decide what happens when AI is unavailable, when images fall outside specs, or when the model is uncertain. Require an explicit “AI reviewed” indicator, log disagreements, and create a quick pathway for feedback so recurring false positives (e.g., hardware, post-op change) get tracked. These controls take time, IT effort, and governance, but they prevent silent drift.
Safety, bias, and regulation: accuracy for every patient group
A typical deployment surprise is that “overall accuracy” can hide uneven safety. Models often perform best on the majority populations and protocols they saw most in training, then degrade in pediatrics, very elderly patients, different body habitus, or in groups underrepresented in the dataset. The practical risk is not just fairness in the abstract; it is differential false negatives and delayed care, or differential false positives and avoidable downstream imaging.
Ask for subgroup performance with confidence intervals, not a single pooled AUC. Confirm how the vendor monitored bias, what data were used for external validation, and whether post-market surveillance is in place. Regulatory clearance is a baseline, not a guarantee of performance in your scanners and workflow; local validation, drift monitoring after upgrades, and a clear incident-reporting pathway add cost and time, but they are what make “accuracy” safe for every patient you serve.
Making AI accuracy gains stick: a checklist for next steps
When a vendor says “we’re more accurate,” translate that into a pilot plan with exit criteria. Start with one use case, one modality, and a defined population; set target thresholds for sensitivity and false-positive volume, plus a fallback process when AI is down or uncertain. Validate locally on your scanners and protocols, then track performance after software, PACS, or reconstruction changes. Budget for integration and training time, and assign ownership for incident review, subgroup monitoring, and feedback loops so recurring errors get fixed rather than normalized.